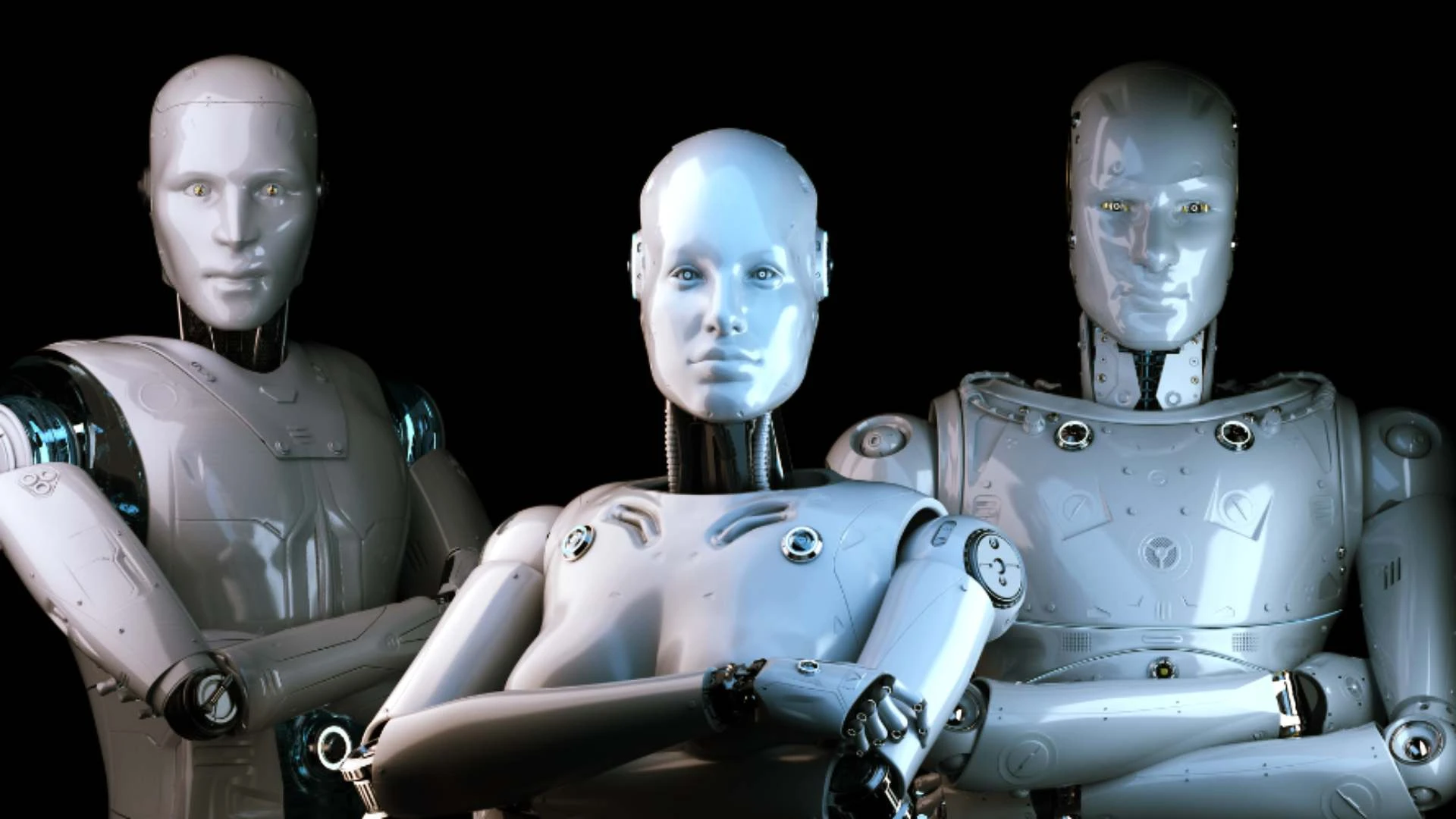
In a groundbreaking leap for robot-kind, we now have robots that can grow by munching on their fellow machines! Forget about the age-old dilemma of "to eat or be eaten"; it seems our metallic friends have opted for the buffet approach. Who knew that the future of robotics would be a culinary adventure? Maybe next we’ll see them in Michelin-starred restaurants, serving up a delightful ‘Cyborg à la Mode’.
Just imagine the conversations at tech conferences: "So, did your robot eat any interesting models this week?" It’s a brave new world, where survival of the fittest has turned into a feast of the fittest.
Bon appétit, little transformers!
#Robotics #AI #TechTrends #
Just imagine the conversations at tech conferences: "So, did your robot eat any interesting models this week?" It’s a brave new world, where survival of the fittest has turned into a feast of the fittest.
Bon appétit, little transformers!
#Robotics #AI #TechTrends #
In a groundbreaking leap for robot-kind, we now have robots that can grow by munching on their fellow machines! Forget about the age-old dilemma of "to eat or be eaten"; it seems our metallic friends have opted for the buffet approach. Who knew that the future of robotics would be a culinary adventure? Maybe next we’ll see them in Michelin-starred restaurants, serving up a delightful ‘Cyborg à la Mode’.
Just imagine the conversations at tech conferences: "So, did your robot eat any interesting models this week?" It’s a brave new world, where survival of the fittest has turned into a feast of the fittest.
Bon appétit, little transformers!
#Robotics #AI #TechTrends #